January 2017 brings the second part of information on gangs, the start of a series on urinalysis (specific gravity this month), an update on resus council guidelines and a link to expressing breastmilk. Do leave comments below.
Tag Archives: APLS
Invasive Group A Strep (GAS) and chicken pox
With thanks to Dr Kat Smith, education fellow and paediatric registrar at King’s College Hospital who answered my call last month for more writers to help me put together the monthly Paediatric Pearls newsletters.
Group A Streptococcal Infection in Chickenpox
Chickenpox in children is common and usually follows a mild and self-limiting (if somewhat itchy) course. After an incubation period of 10-21 days the first signs of illness are viral prodrome, mild pyrexia, and the classic cropping vesicular rash; the pyrexia is typically mild (38-39oC) and lasts 3-4 days.
In otherwise healthy children the most common complication of chickenpox is secondary bacterial skin infection, typically caused by scratching lesions. Whilst most of these are mild impetigo or localised cellulitis, the increased incidence of group A streptococcal (GAS) colonisation in children (around 10% are asymptomatic carriers in the throat or on skin) makes invasive GAS infection a real concern.
Secondary bacterial skin infection
This is characterised by erythema +/- tenderness around lesions. Children may be well in themselves if the infection is superficial; if they become more unwell this raises the suspicion of a more serious or invasive bacterial infection.
Serious bacterial superinfection / Invasive GAS infection
Around a third of children admitted to hospital with chickenpox have secondary skin infection, some of whom develop invasive infections such as pneumonia, osteomyelitis and septicaemia. GAS in particular can be associated with more fulminant infectious processes such as necrotising fasciitis and toxic shock syndrome (TSS); both are associated with high mortality and morbidity in children.
Features that should prompt consideration of a serious bacterial superinfection are:
- A lethargic or unwell-looking child; remember, children with chickenpox are typically uncomfortable but well.
- Spiking, high-grade pyrexia
- Pyrexia for longer than 4 days, particularly after initial improvement
- Diarrhoea or vomiting
- Soft tissue pain which seems disproportionate to other examination findings (an early sign of necrotising fasciitis)
How to prevent bacterial superinfection
Because scratching lesions is the most likely way to allow bacteria to breach the body’s normal defences, the primary aim of prevention is to limit scratching:
- Keep skin moisturised. Many parents still use calamine lotion but it is worth noting that it becomes ineffective once dry, and traditional emollients (e.g. 50:50) may be more effective.
- There is evidence that sedating antihistamines offer some benefit; chlorphenamine is licensed for this use.
- Dress children in smooth, loose, cotton clothing.
- Keep fingernails trimmed short.
- There are rare reports of NSAIDs potentially worsening skin infections in chickenpox, so ibuprofen should be used with caution. In practice, it would be unusual for a child to need ibuprofen if receiving regular paracetamol; pain or pyrexia necessitating its use in addition to paracetamol should prompt consideration of serious bacterial superinfection.
- There is no evidence to support the use of acyclovir in young, immunocompetent children with self-limiting, uncomplicated chickenpox; it does not decrease the incidence of complications.
What to do if you suspect bacterial superinfection
- Otherwise well children with evidence of few, small areas of bacterial superinfection can be managed in the community with oral antibiotics and safety-netting advice.
- Children with evidence of collection, extensive areas of bacterial superinfection, who are unwell, or have other features consistent with possible serious bacterial superinfection, need urgent referral to secondary care.
- In secondary care, unwell children with evidence of shock / sepsis need urgent resuscitation and intravenous antibiotic administration; if possible this should include clindamycin, due to its vital role in inhibiting toxin production by GAS.
- Invasive GAS infection has high mortality, and if suspected there should be a low threshold to involve senior staff, regional PICU services, and in the case of necrotising fasciitis, surgical teams (for early debridement); early use of inotropes and IVIG may also be required.
Bibliography
Chickenpox NICE Clinical Knowledge Summary (which I found to be the best resource by far): http://cks.nice.org.uk/chickenpox
Cohen J, Breuer J. Chickenpox treatment. Systematic review 912. BMJ Clinical Evidence.
Papadopoulos, AJ. Chickenpox. emedicineWebMD. www.emedicine.com
References
Re: “the increased incidence of group A streptococcal (GAS) colonisation in children (around 10% are asymptomatic carriers in the throat or on skin)”
Shaikh N, Leonard E, Martin JM. Prevalence of streptococcal pharyngitis and streptococcal carriage in children: a meta-analysis. Pediatrics. 2010 Sep;126(3):e557-64
Re. “Around a third of children admitted to hospital with chickenpox have secondary skin infection”:
Bovill B, Bannister B. Review of 26 years/ hospital admission for chickenpox in North London. Journal of Infection. 1998;36(suppl1);17-23.
Re: “necrotising fasciitis and toxic shock syndrome (TSS); both are associated with high mortality and morbidity in children.” AND “IVIG may also be required.”
Chuang YY, Huang YC, Lin TY. Toxic shock syndrome in children: epidemiology, pathogenesis, and management. Paediatr Drugs. 2005;7(1):11-25.
Re. “There is evidence that sedating antihistamines offer some benefit”
Tebruegge M, Kuruvilla M, Margarson I. Does the use of calamine or antihistamine provide symptomatic relief from pruritus in children with varicella zoster infection? Archives of Disease in Childhood. 2006:91(12);1035-1036.
Re: (continued from above) “chlorphenamine is licensed for this use.”
BNFC, available at: https://www.medicinescomplete.com/mc/bnfc/current/PHP1934-chlorphenamine-maleate.htm?q=chlorphenamine&t=search&ss=text&tot=40&p=1#_hit
Re: “if possible this should include clindamycin, due to its vital role in inhibiting toxin production by GAS.” (as well as having it drilled in to us by the microbiologists at St Thomas’):
http://emedicine.medscape.com/article/228936-medication#2
March 2015 published
March 2015: the first post of the new ENT feature this month – glue ear, more help with viral exanthems, important safeguarding information on the UK government’s Prevent Strategy, breastfeeding for mums and research in the paediatric ED.
February 2015 (just)
Have just uploaded February 2015 newsletter – with 4.5 hours of February to go….
NICE on gastro-oesophageal reflux disease, how to recognise speech delay, more viral exanthems, resus cards and information on forthcoming allergy courses. Do leave comments below:
July 2014 published
Last bit of headaches this month with guidance on management of various primary headaches, including medication overuse headache. Also more on domperidone, psoriasis, respiratory and heart rates to worry about and a link to a new colic summary I’ve put under the Primary Care Guidelines tab. Do leave comments below.
March 2013 up and running
Delayed sleep phase this month and chronotherapy which sounds like quite an undertaking. Also a link to a new parent’s guide to picking up and talking about sexual abuse, links to handy recent uploads to the site, the BSACI guideline on allergic rhinitis and more banging on about vitamin D supplementation – please.
Dr Noimark’s allergy management plans
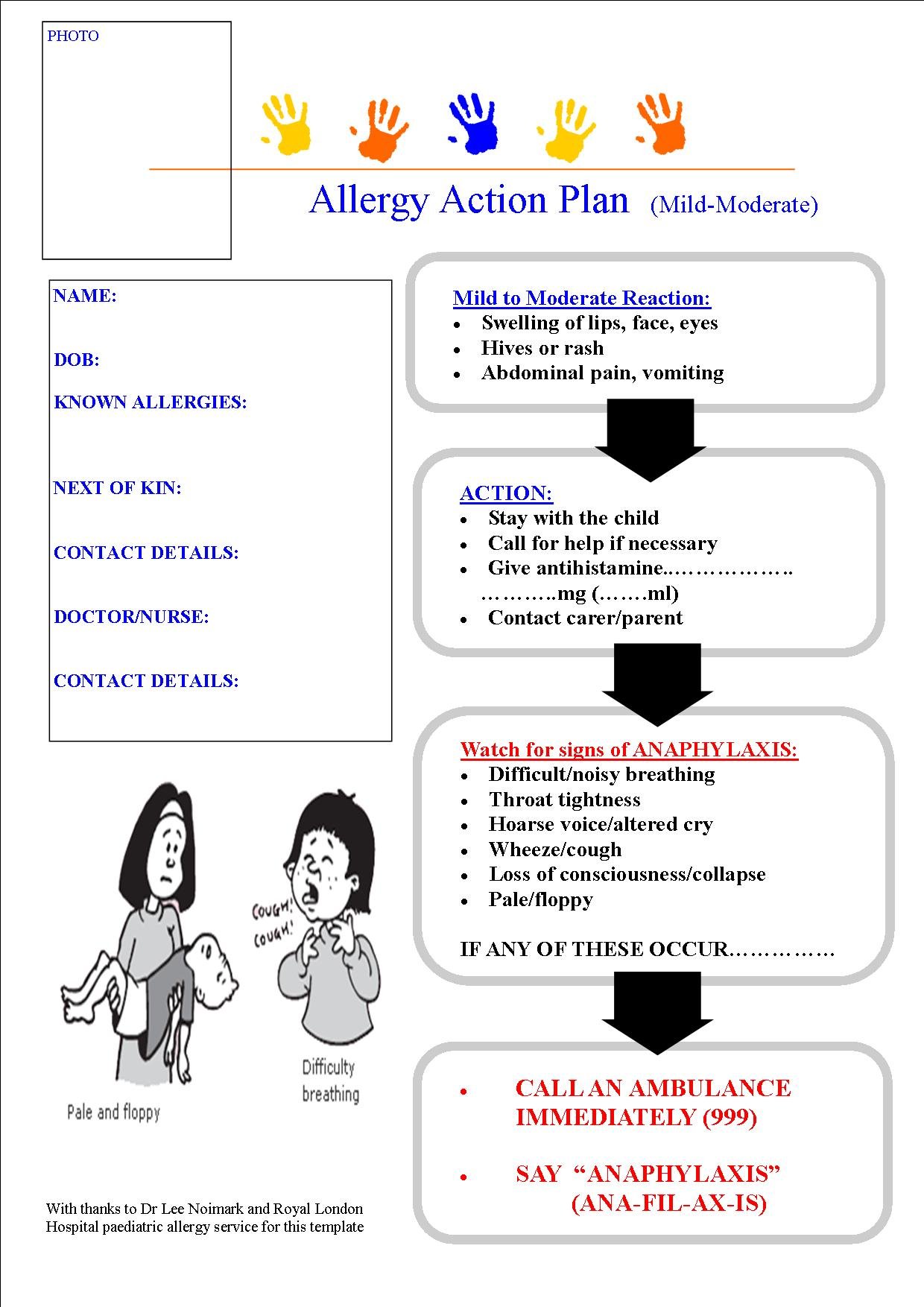
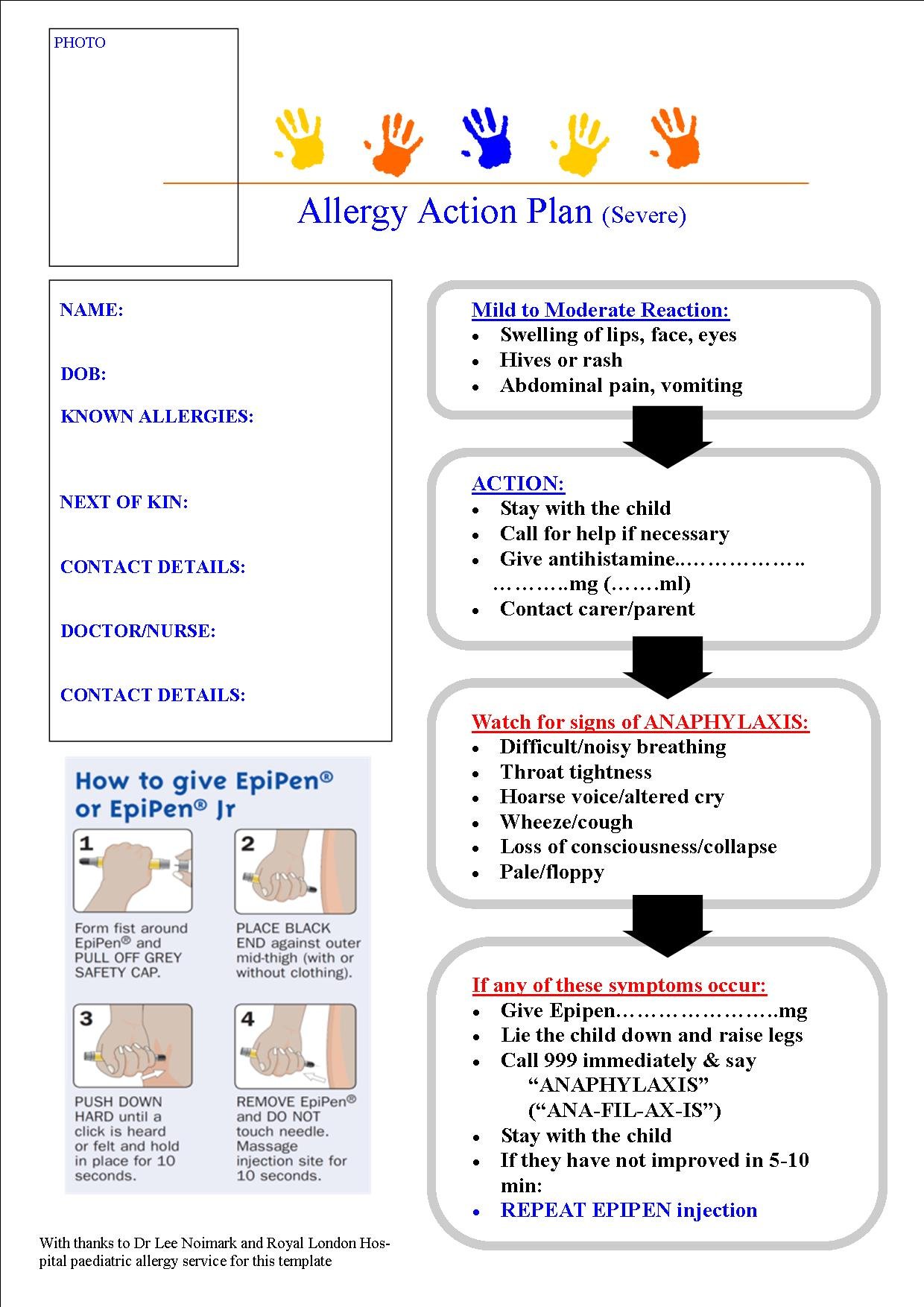
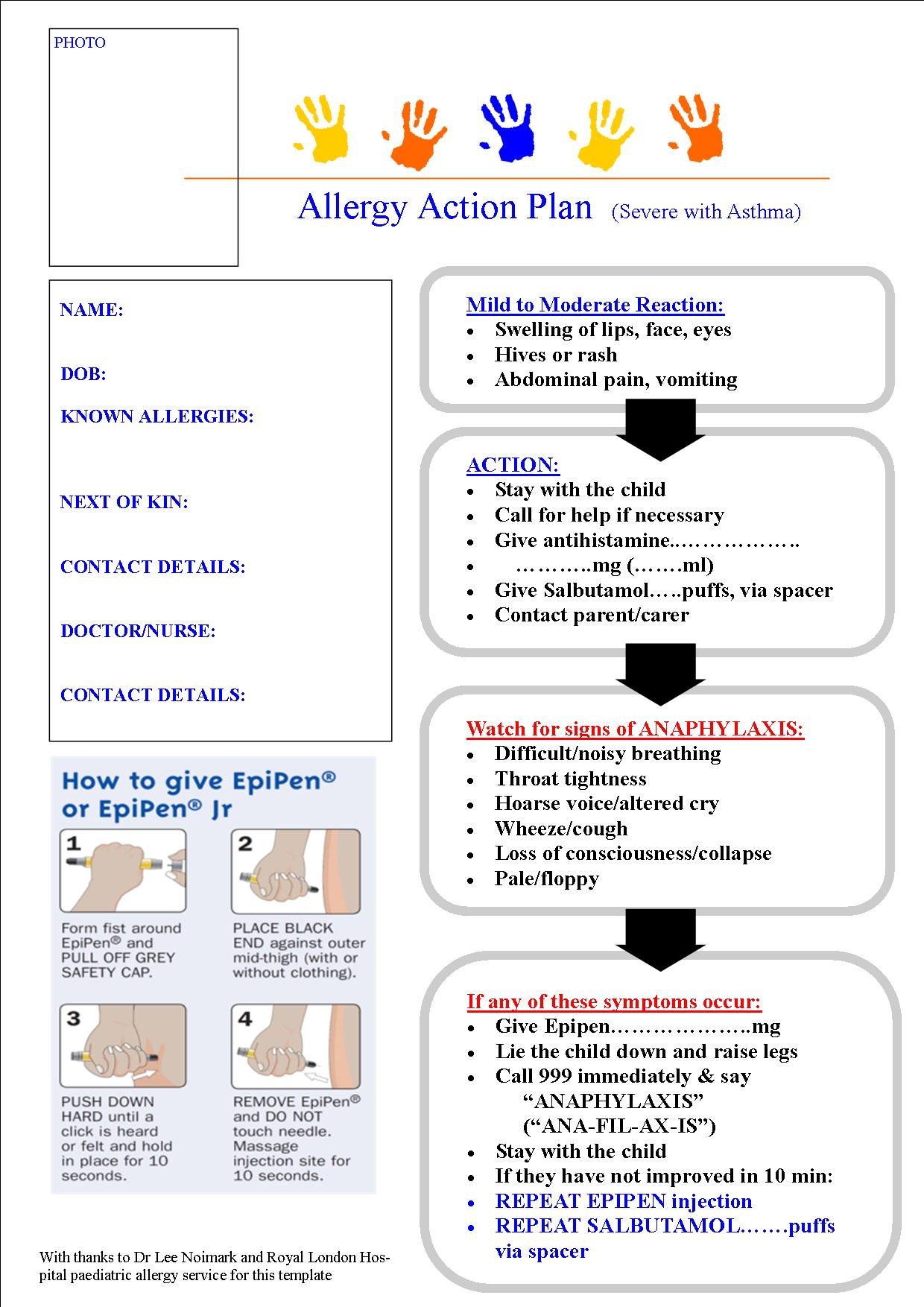
Lee Noimark is a paediatric allergist at the Royal London Hospital. He and his team put these allergy action plans together. Print them out for your patients to give to nursery or school in the event of an allergic reaction. The labels are self explanatory:
Allergy Action Plan (mild-moderate)
{kind=link}
Allergy Action Plan (mild-moderate with asthma)
{kind=link}
{kind=link}
Allergy Action Plan (severe with asthma)
{kind=link}
November 2012 published!
The common assessment framework triangle for assessing children in need this month with some tips on how to press the right buttons with children’s social care referrals. Also a bit on stabilisation and transfer for the ED teams, a reminder not to use 0.18% saline and the start of a minor injuries series. Talipes for the GPs and paediatricians among you.
October 2012 ready to go!
Coins, magnets and batteries on the menu this month as well as some more cows milk protein allergy resources. A reminder about child developmental milestones courtesy of one of our medical students and NICE on headaches. Do leave comments!
Foreign body ingestion
The information for this topic is taken from a recent comprehensive review (August 2012) that appeared in www.UpToDate.com. Bartshealth employees can access the full text via a link from the intranet.
Ingested foreign bodies (UptoDate.com article, August 2012)
Coins — Coins are by far the most common foreign body ingested by children. Approximately two-thirds of ingested coins are in the stomach by the time of x-ray but those that lodge in the oesophagus for 24 hours after ingestion may need to be removed endoscopically as only 20-30% of these will pass into the stomach on their own. Coins that reach the stomach can be managed expectantly, and most will be passed within one to two weeks. A child who develops any signs or symptoms of obstruction, abdominal pain, vomiting, or fever, needs to come back to the ED urgently.
Button batteries — ingestions of “button” batteries are increasing and are associated with significant morbidity. Animal studies have demonstrated mucosal necrosis within one hour of ingestion and ulceration within two hours, with perforation as early as eight hours after ingestion. It may be difficult to differentiate between a disk battery and a coin on a radiograph. This distinction is most important when the foreign body is in the oesophagus, since batteries require immediate removal whereas coins may not.
Magnets — also increasing. Many of the children with complications from multiple magnet ingestion had underlying developmental delay or autism. In one case, an older child inadvertently swallowed these magnets while using them to imitate a pierced tongue. Two or more strong magnets, especially if ingested at different times, may attract across layers of bowel leading to pressure necrosis, fistula, volvulus, perforation, infection, or obstruction. Radiographs of the neck and abdomen should be performed, including a lateral view. X-rays cannot usually determine whether bowel wall is compressed between the magnets, although the finding of magnets that appear to be stacked but are slightly separated is suggestive. Management depends on the number, location and type of magnets, and on the timing of the ingestion. Ingestion of a single magnet can generally be managed conservatively with serial radiographs while multiple magnets need removing. Laxatives may help with faster bowel emptying if they are not in a place easily accessible with the endoscope.
References at www.uptodate.com.