From left to right: Dubsmash (high risk of bullying), Snapchat (overall safety rating – average), Smule (official age rating 13+), We chat (high risk sexual and bullying), Twitch (“it’s hard to censor because it’s live”), YouTube (“people write mean things in the comments on videos”). Follow the links to read about each site’s safety profile and find out what kind of thing your own children and your young patients are using the individual sites for.
Social media sites are here to stay and preventing children having access to them is not likely to be a successful parental pastime. https://www.net-aware.org.uk/ is an O2 and NSPCC project which looks at the safety of social media sites and gives parents tips on how to protect their children while they are using them.
Acute Kidney Injury (AKI) by Alex Argyropoulos this month: risk, recognition and management. Surgical update on hernias, the difficulties of wearing masks for people who stutter and a helping hand from Harry the Hound for children worried about going back to school after covid.
Safeguarding again this month. Youth Violence Commission final report, sweets laced with cannabis oil, trauma-informed care and links to 2 excellent sites demonstrating disparity and deprivation through images. Do leave comments below.
Remote assessment of children the Wessex way this month, tight foreskins, difficult airways and a journal club discussion around the likelihood of meningitis in neonatal UTI. Do leave comments below…
Lots of useful Child Safeguarding resources in this month’s newsletter. Neglect of medical needs, more Covid 19 resources, support for new parents and plenty of links to on line resources to help you keep your safeguarding CPD log books up to date. Do leave comments below:
April 2020: The start of “surgical paediatric pearls” series this month, a reminder that the NHS is open for children during the COVID period, DKA update and frontline assessment of anorexia nervosa. Do leave comments below:
With thanks to Dr Ed Dallas, paediatric registrar, for putting together a succinct guide to eating disorders and the management of re-feeding syndrome.
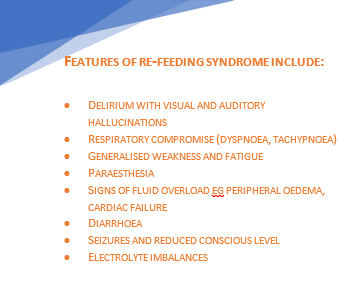
Re-introduction of nutrition to severely malnourished individuals can precipitate refeeding syndrome which may result in cardiac failure and death.
The key biochemical abnormality is hypophosphataemia, due to total body phosphate depletion and a shift of extracellular to intracellular phosphate when the body changes from a catabolic state to anabolic.
The risk is greatest in the initial stages of refeeding (first week). The incidence increases with decreasing BMI and if weight loss is rapid.
Anorexia is a serious, potentially fatal disease—while refeeding syndrome can be fatal, the risk from malnutrition and ‘underfeeding’ is much greater.
In A&E:
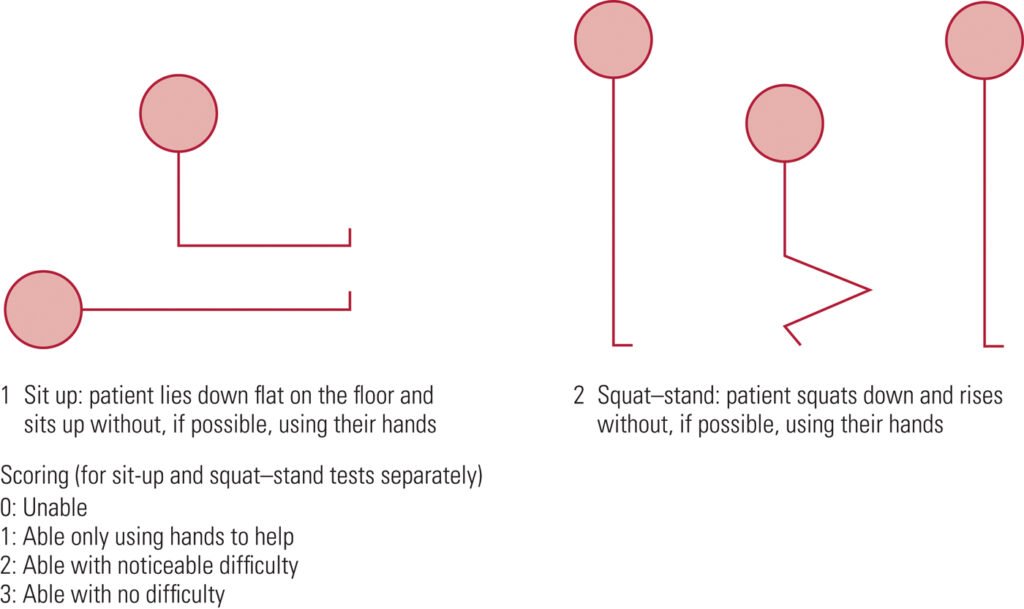
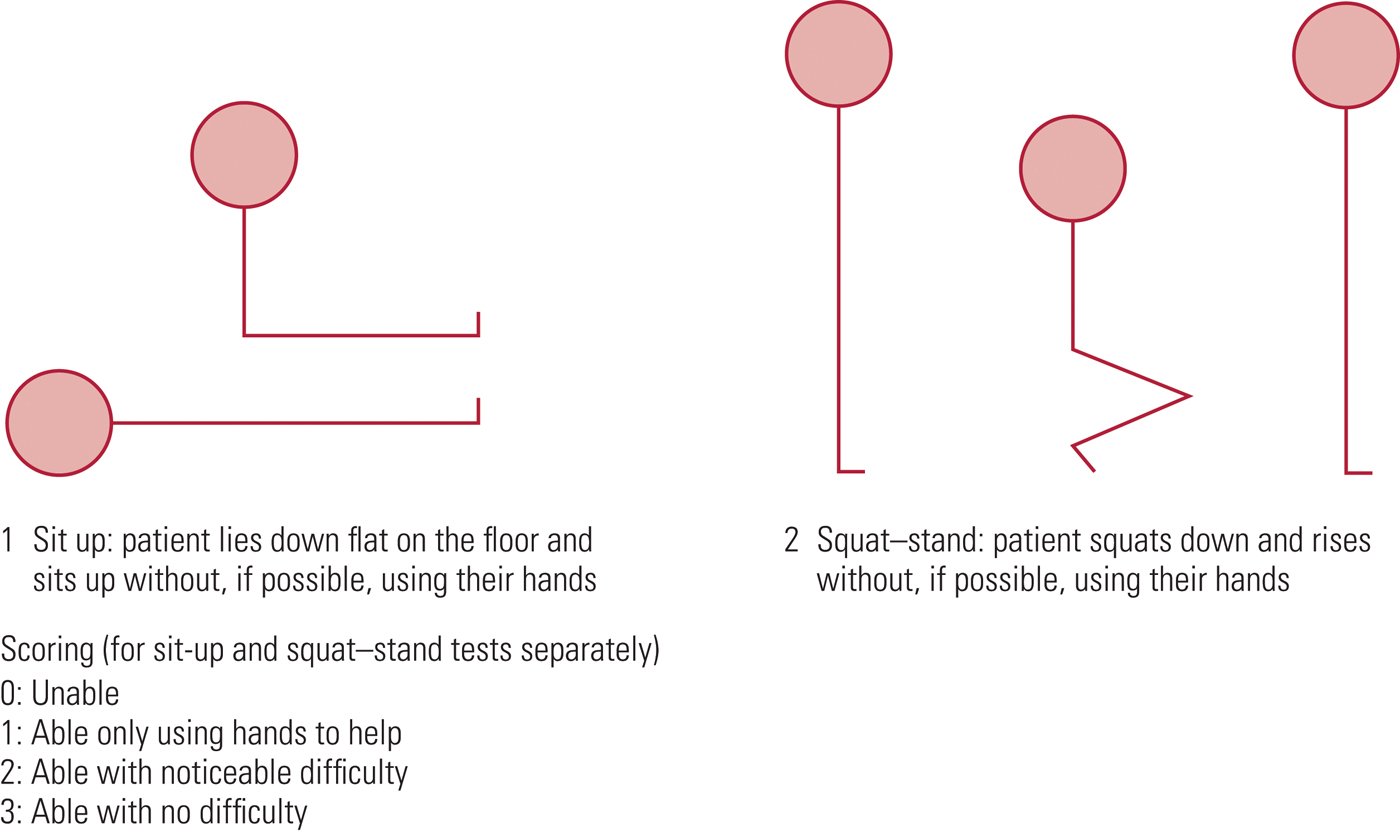
– Assess using SCOFF questionnaire and Sit-up/Squat test.
– Consider differentials for weight loss in children (e.g. Malignancy, hormonal, illness)
– Risk Assessment according to Junior MARSIPAN guidelines: Clinical parameters, location of care, compulsory admission/treatment, legislation (e.g. Gillick competence, Mental Health Act)
See Summary below of what to look for and when to be concerned!
Once admitted:
Baseline bloods: Red flags: Na+ < 130mmol/L, K+ < 3mmol/L, Phosph < 0.5mmol/L often symptomatic if phosphate <1mmol/L (range 1.3-2.1mmol/L), Glucose
ECG (look specifically for prolonged QTc)
For children, use the percentage of 50th centile BMI, not just the BMI.*
All vital signs, however, are to be checked against standardcharts for their age. Patients can be hypotensive, bradycardic, hypothermic.
*Plot BMI on growth chart. To calculate percentage median BMI:
Percentage BMI = actual BMI (weight/height2) x 100
median BMI (50th percentile) for age & gender
Treatment & Re-feeding:
Patient should be fed in as normal a fashion as possible. If this fails, NG feeds should be considered early in the admission. Make the decision within 24 hours. Specialist paediatric dietician must be involved early.
Risk from Re-feeding Syndrome can be reduced by careful monitoring and paediatric dietician input into choice of feed composition. A diet too high in carbohydrates increases the risk of re-feeding syndrome.
Consider phosphate (and other) supplementation early. Replace and titrate according to bloods which should be taken just before the supplement is given. Stores are usually replenished after 1 week but continue for at least 2 weeks. Consider long term lower dose supplementation.
Re-feeding Bloods (U&Es, LFTs, Phosphate, Calcium, Magnesium) to be taken before re-feeding, 6 hours after starting and then daily for 2-5 days, then at 7-10 days, at least until 2 weeks. Ideally, bloods to be taken just before any supplementation are given (so levels are not falsely high).
Patients should not be ‘underfed’ for fear of refeeding syndrome: consider starting at 20 kcal/kg/day, 5-10kcal/kg/day if high risk
CAMHS
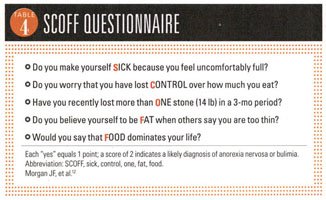
SCOFF questionnaire for screening Anorexia and Bulimia
Shown to have 100% sensitivity and a specificity of 89% for patients with anorexia and bulimia.
*One point for every “yes”
A score of ≥2 indicates a likely case of anorexia nervosa or bulimia
Young people with an eating disorder may deny all the above, in which case it is very important to use your clinical judgement, monitor the situation and provide follow-up.
SUSS Test – see diagram below
Those who are High risk for re-feeding syndrome
Very low percentage median body mass index
Minimal or no nutritional intake for the past 3–4 days
Weight loss >15% in the past 3 months
Abnormal electrolytes prior to starting re-feeding
→ May need a more cautious approach (5–10 kcal/ kg/day starting regimen) with twice daily bloods
Refeeding Plan:
Paediatric dietician for specialist advice.
Correct dehydration – usually over 48 hours as too rapid correction can result in cardiac decompensation
Prescribe multivitamin and mineral supplements; consider thiamine in older children. Start any multivitamins and mineral supplementations before feeding begins (NICE CG9)
Refeeding should ideally mimic normal eating
If the patient cannot comply with a meal plan then NG considered by 24 hours. Use a daytime bolus regimen to mimic physiological eating
Consider starting at 20 kcal/kg/day. Aim for 0.5–1 kg/week weight gain.
To prevent underfeeding—aim to increase by 200 kcal/day until full nutritional requirements for weight gain are achieved (this should be within 5–7 days).
If hypophosphataemia develops, maintain rather than reduce calorie intake; consider supplementation.
Daily Re-feeding bloods (U&Es, LFTs, phosphate, magnesium) during the ‘at-risk’ period of days 2–5 initially, and at 7– 10 days (to identify late refeeding syndrome) up to at least 2 weeks
Restrict carbohydrate intake and increase dietary phosphate (eg, using milk). If NG feeding, avoid high calorie concentration feeds (high carbohydrate content increases the risk of re-feeding syndrome).
WHAT SHOULD I START DOING?
Assess nutritional status based on percentage median BMI, and not BMI alone.
Baseline clinical assessment of risk includes baseline ECG and SUSS test for weakness.
Have a low threshold for starting NG feeding and avoid an overcautious approach to re-feeding (consider starting at 20 kcal/kg/day and increasing by 200 kcal/day until nutrition is sufficient for weight gain).
Always consider re-feeding syndrome—monitor patient’s electrolytes (especially phosphate) before and during re-feeding, and assess the risk of re-feeding syndrome prior to starting feeding.
Prescribe a general vitamin and mineral supplement in younger children, and consider thiamine supplements in older children (main evidence in adults).
WHAT SHOULD I STOP DOING?
Taking an overcautious approach to re-feeding (may result in underfeeding syndrome)—patients should be receiving sufficient nutrition for weight gain within 5–7 days of re-feeding.
For patients receiving supplemental or NG feeds, avoid calorie dense feeds, which may be too high in carbohydrates and increase the risk of re-feeding syndrome.
March has been guest edited by Dr Jackie Driscoll, Academic GP and erstwhile paediatric registrar. Jackie was keen to produce a newsletter which centres on the child but sees them in the context of their family, their school and neighbourhood.
Burns this month – with much discussion amongst the editorial group prior to publication. There are lots of different children’s burns protocols it transpires. RCEM’s is not aligned with the London and South East Burns Network’s. The message is “use your own burns referral unit’s guideline”. The other important message about burns is watch out for NAI but, even if the burn is accidental, refer all children to their health visitor as HVs in the UK are responsible for talking to families about safety in the home.
Also, complications of Kawasaki Disease, ADHD and the updated MAP guideline (managing cows milk allergy in primary care) which emphasises that 98% of crying babies do not have CMPA. Do leave comments below.
ADHD is a chronic life long disorder of self-regulation with symptoms persisting in >70-80% adolescents and >50% adults.
It is real disorder with real long-term risks, just to quote a few impacts….
Up to 30% of children may have depression and up to half of girls with ADHD may attempt self-harm
Children with untreated ADHD are >5 times more likely to participate in fights and underachieve at school
Adults with ADHD are 9 times more likely to end up in prison, more likely to experience financial problems and being fired from a job.
Adults with ADHD have a higher mortality compared to those without mainly due to causes such as driving accidents, substance abuse, obesity and co-morbid problems (Dalsgaard et al. Lancet 2015, May;385(9983):2190-6)
Red Flags:
Organisational skills problems (time management, memory, late and unfinished homework and projects)
Erratic work and academic performance
Family/marital problems
Poor sleep and other household routines
Difficulty managing finances, impulsive shopping
Compulsive addictions – sex, gambling, video gaming, exercise, eating
Frequent accidents secondary to recklessness
Speeding tickets, car and motorbike accidents
First degree relatives with ADHD
Low self-esteem, chronic under-achievement
ADHD is usually diagnosed after the age of 6 years to allow for the child to mature. Almost all children have times when their behaviour seems unacceptable and age inappropriate. However, when behaviours happen many times a week or daily, ADHD ought to be looked for. NICE guidance allows children to be treated after the age of 5 years and medication makes a huge and quick difference along with psychoeducation and behavioural management.
Resources: The Canadian ADHD Resource Alliance (www.caddra.ca is an excellent resource for professionals with free downloads).
US guidelines have recently changed to allow treatment of some 4 year olds with debilitating features of ADHD (https://www.healthychildren.org/English/news/Pages/Practice -Guideline-for-the-Diagnosis-Evaluation-and-Treatment-of- ADHD.aspx)
To provide the best experiences, we use technologies like cookies to store and/or access device information. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional
Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.