This month‘s newsletter has a child safeguarding theme, with thanks to Dr Jackie Driscoll who edited it this month. A round up of educational and support resources for us and our patients and their families.

This month‘s newsletter has a child safeguarding theme, with thanks to Dr Jackie Driscoll who edited it this month. A round up of educational and support resources for us and our patients and their families.
This month‘s newsletter has some helpful resources for parents of children of all ages. Also a reminder from Islington borough of London that children should be at school if they have minor illnesses. Everyone gets muddled up with HSP and ITP so we’ve put together a comparison table. Do leave comments below…

Lots about diarrhoea this month. Also ADHD and no need any more for an ECG prior to starting medication. Obesity in A&E; can we at least start the journey towards a more healthy future in the Emergency department?

Useful resources in preparation for this year’s expected RSV bronchiolitis surge in this month’s newsletter. Also, a bit on managing young people who are “tired all the time”, height and weight issues in non face-to-face consultations and a short article asking why do we give children 10 days of foul tasting pen-V qds for tonsillitis instead of 5 days of tds amoxicillin which, it transpires, is actually cheaper? Microbiologists and others are welcome to leave comments below!
Digging deep into safeguarding again this month with thanks to Nicci Wotton, head of safeguarding at Imperial, London, UK. A reminder of useful apps for our young patients and pointers to documents that govern our safeguarding responsibilities in the UK and internationally. Do leave comments below.

Testicular torsion this month – a surgical emergency with good outcomes if operated on less than 6 hours since the pain started.
Also, links to helpful health and well being websites for young people and to good ECG CPD for psychiatrists and GPs. A bit more on ADHD and a round up of neck lumps in infants, assessment and management.
Do leave comments below.
Lots of useful Child Safeguarding resources in this month’s newsletter. Neglect of medical needs, more Covid 19 resources, support for new parents and plenty of links to on line resources to help you keep your safeguarding CPD log books up to date. Do leave comments below:
April 2020: The start of “surgical paediatric pearls” series this month, a reminder that the NHS is open for children during the COVID period, DKA update and frontline assessment of anorexia nervosa. Do leave comments below:
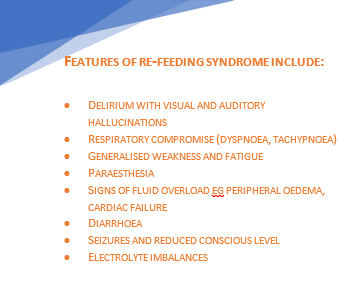
With thanks to Dr Ed Dallas, paediatric registrar, for putting together a succinct guide to eating disorders and the management of re-feeding syndrome.
Re-introduction of nutrition to severely malnourished individuals can precipitate refeeding syndrome which may result in cardiac failure and death.
The key biochemical abnormality is hypophosphataemia, due to total body phosphate depletion and a shift of extracellular to intracellular phosphate when the body changes from a catabolic state to anabolic.
The risk is greatest in the initial stages of refeeding (first week). The incidence increases with decreasing BMI and if weight loss is rapid.
Anorexia is a serious, potentially fatal disease—while refeeding syndrome can be fatal, the risk from malnutrition and ‘underfeeding’ is much greater.
In A&E:
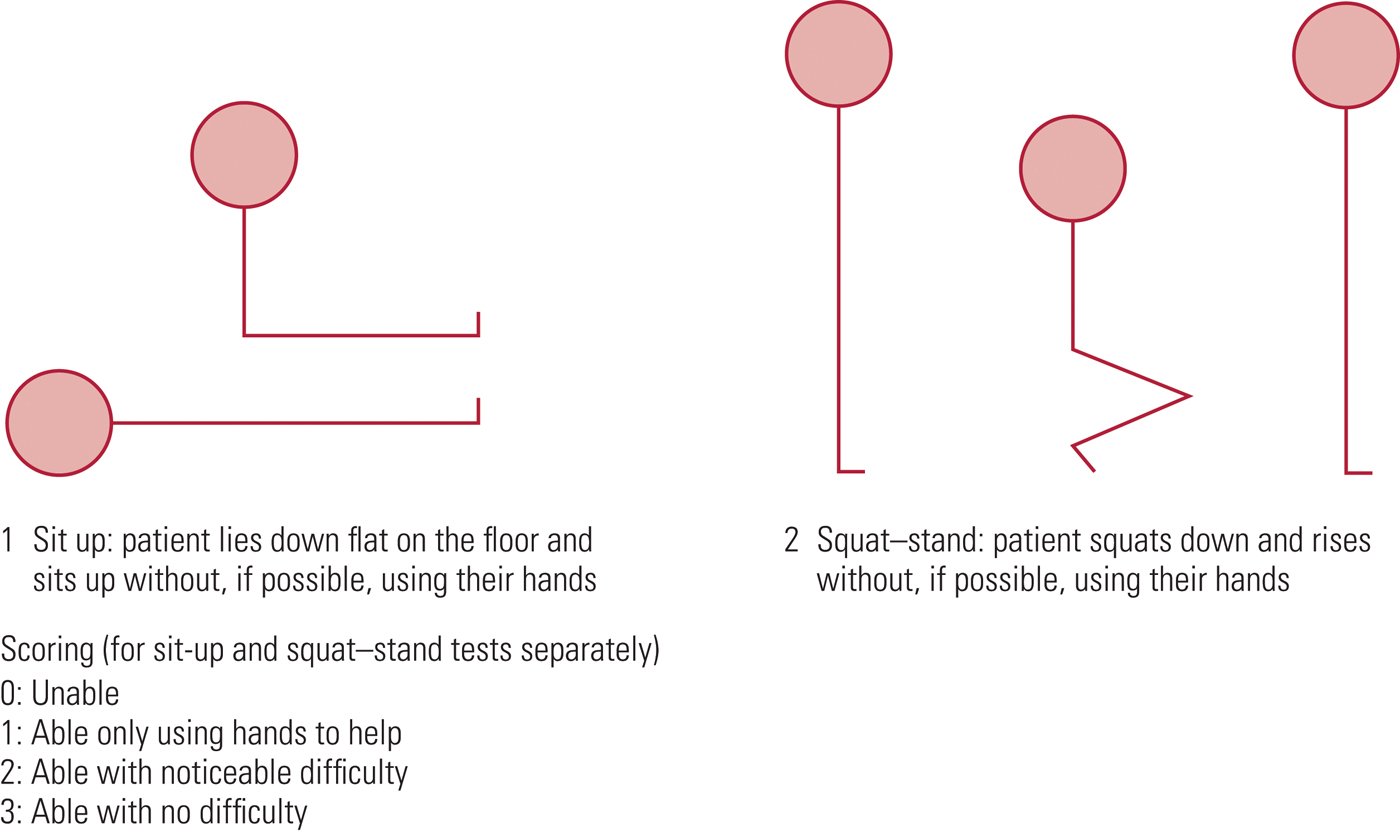
– Assess using SCOFF questionnaire and Sit-up/Squat test.
– Consider differentials for weight loss in children (e.g. Malignancy, hormonal, illness)
– Risk Assessment according to Junior MARSIPAN guidelines: Clinical parameters, location of care, compulsory admission/treatment, legislation (e.g. Gillick competence, Mental Health Act)
See Summary below of what to look for and when to be concerned!
Once admitted:
*Plot BMI on growth chart. To calculate percentage median BMI:
Percentage BMI = actual BMI (weight/height2) x 100
median BMI (50th percentile) for age & gender
Treatment & Re-feeding:
Patient should be fed in as normal a fashion as possible. If this fails, NG feeds should be considered early in the admission. Make the decision within 24 hours. Specialist paediatric dietician must be involved early.
Risk from Re-feeding Syndrome can be reduced by careful monitoring and paediatric dietician input into choice of feed composition. A diet too high in carbohydrates increases the risk of re-feeding syndrome.
Consider phosphate (and other) supplementation early. Replace and titrate according to bloods which should be taken just before the supplement is given. Stores are usually replenished after 1 week but continue for at least 2 weeks. Consider long term lower dose supplementation.
Re-feeding Bloods (U&Es, LFTs, Phosphate, Calcium, Magnesium) to be taken before re-feeding, 6 hours after starting and then daily for 2-5 days, then at 7-10 days, at least until 2 weeks. Ideally, bloods to be taken just before any supplementation are given (so levels are not falsely high).
Patients should not be ‘underfed’ for fear of refeeding syndrome: consider starting at 20 kcal/kg/day, 5-10kcal/kg/day if high risk
CAMHS
SCOFF questionnaire for screening Anorexia and Bulimia
Shown to have 100% sensitivity and a specificity of 89% for patients with anorexia and bulimia.
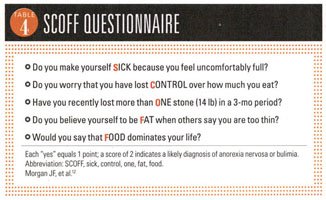
*One point for every “yes”
A score of ≥2 indicates a likely case of anorexia nervosa or bulimia
Young people with an eating disorder may deny all the above, in which case it is very important to use your clinical judgement, monitor the situation and provide follow-up.
SUSS Test – see diagram below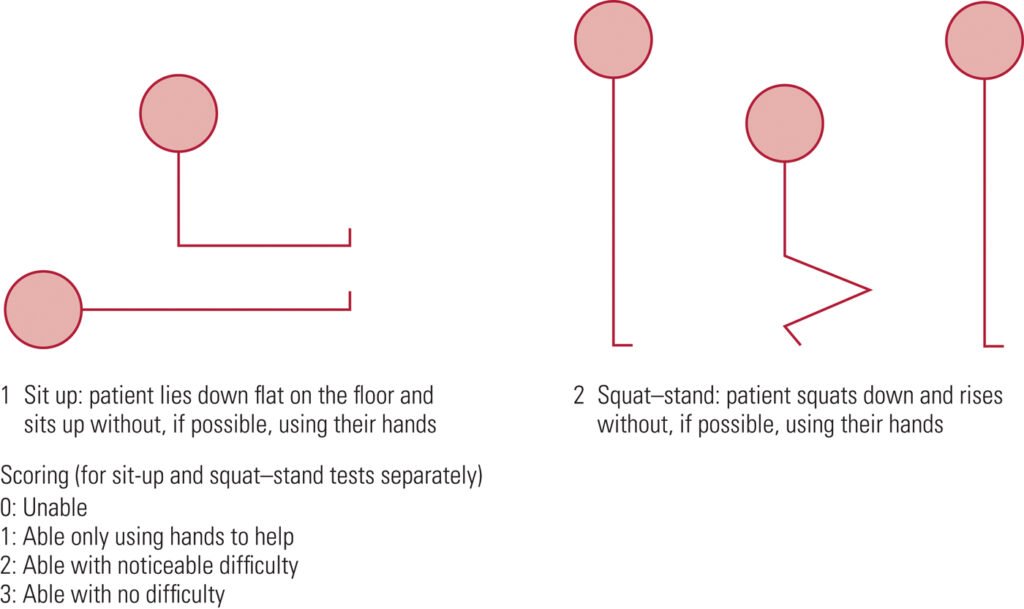
Those who are High risk for re-feeding syndrome
→ May need a more cautious approach (5–10 kcal/ kg/day starting regimen) with twice daily bloods
Refeeding Plan:
WHAT SHOULD I START DOING?
WHAT SHOULD I STOP DOING?
Useful Summary of Marsipan guidelines from BMJ:
https://ep.bmj.com/content/edpract/early/2015/09/25/archdischild-2015-308679.full.pdf?keytype=ref&ijkey=zgb4e3x2vGIWEmL
Link to FULL Junior Marsipan Guidance from RCPSYCH (75 page PDF):
https://www.rcpsych.ac.uk/docs/default-source/improving-care/better-mh-policy/college-reports/college-report-cr168.pdf?sfvrsn=e38d0c3b_2
Medical Management of Anorexia Nervosa:
Managing Anorexia; BMJ Review:
https://adc.bmj.com/content/96/10/977
Hypophospataemia in Anorexia Nervosa; BMJ review:
https://pmj.bmj.com/content/77/907/305.full
with thanks to Dr Monika Bajaj, neurodevelopmental paediatrician practising privately in east London.
ADHD is a chronic life long disorder of self-regulation with symptoms persisting in >70-80% adolescents and >50% adults.
It is real disorder with real long-term risks, just to quote a few impacts….
Red Flags:
ADHD is usually diagnosed after the age of 6 years to allow for the child to mature. Almost all children have times when their behaviour seems unacceptable and age inappropriate. However, when behaviours happen many times a week or daily, ADHD ought to be looked for. NICE guidance allows children to be treated after the age of 5 years and medication makes a huge and quick difference along with psychoeducation and behavioural management.
Resources: The Canadian ADHD Resource Alliance (www.caddra.ca is an excellent resource for professionals with free downloads).
US guidelines have recently changed to allow treatment of some 4 year olds with debilitating features of ADHD (https://www.healthychildren.org/English/news/Pages/Practice -Guideline-for-the-Diagnosis-Evaluation-and-Treatment-of- ADHD.aspx)
UK support group: https://www.borntobeadhd.co.uk/