Reintroduction of egg this month with thanks to the BSACI, benign acute childhood myositis, NICE on iv fluids plus a couple of links on when not to use this guidance and a comparison of algorithms for children with a non-blanching rash. Do leave comments below.
Tag Archives: fever
April 2016 PDF digest
April 2016’s offering ripe for reading over the bank holiday weekend. Last text box from the 2014 BTS asthma guideline – this time on acute management, FGM and the importance of reporting colleagues who may be involved in the practice, Group A strep infection as a complication of chicken pox and some links to some good CPD sites for you and your patients.
We also welcome Dr Kat Smith this month, paediatric registrar and education fellow at King’s College Hospital, who has kindly volunteered to write monthly articles for the newsletter. It’s nice to have a fresh pair of eyes on paediatric topics and a fresh nose to the ground so to speak. Thanks, Kat, for your help.
Do leave comments below.
Invasive Group A Strep (GAS) and chicken pox
With thanks to Dr Kat Smith, education fellow and paediatric registrar at King’s College Hospital who answered my call last month for more writers to help me put together the monthly Paediatric Pearls newsletters.
Group A Streptococcal Infection in Chickenpox
Chickenpox in children is common and usually follows a mild and self-limiting (if somewhat itchy) course. After an incubation period of 10-21 days the first signs of illness are viral prodrome, mild pyrexia, and the classic cropping vesicular rash; the pyrexia is typically mild (38-39oC) and lasts 3-4 days.
In otherwise healthy children the most common complication of chickenpox is secondary bacterial skin infection, typically caused by scratching lesions. Whilst most of these are mild impetigo or localised cellulitis, the increased incidence of group A streptococcal (GAS) colonisation in children (around 10% are asymptomatic carriers in the throat or on skin) makes invasive GAS infection a real concern.
Secondary bacterial skin infection
This is characterised by erythema +/- tenderness around lesions. Children may be well in themselves if the infection is superficial; if they become more unwell this raises the suspicion of a more serious or invasive bacterial infection.
Serious bacterial superinfection / Invasive GAS infection
Around a third of children admitted to hospital with chickenpox have secondary skin infection, some of whom develop invasive infections such as pneumonia, osteomyelitis and septicaemia. GAS in particular can be associated with more fulminant infectious processes such as necrotising fasciitis and toxic shock syndrome (TSS); both are associated with high mortality and morbidity in children.
Features that should prompt consideration of a serious bacterial superinfection are:
- A lethargic or unwell-looking child; remember, children with chickenpox are typically uncomfortable but well.
- Spiking, high-grade pyrexia
- Pyrexia for longer than 4 days, particularly after initial improvement
- Diarrhoea or vomiting
- Soft tissue pain which seems disproportionate to other examination findings (an early sign of necrotising fasciitis)
How to prevent bacterial superinfection
Because scratching lesions is the most likely way to allow bacteria to breach the body’s normal defences, the primary aim of prevention is to limit scratching:
- Keep skin moisturised. Many parents still use calamine lotion but it is worth noting that it becomes ineffective once dry, and traditional emollients (e.g. 50:50) may be more effective.
- There is evidence that sedating antihistamines offer some benefit; chlorphenamine is licensed for this use.
- Dress children in smooth, loose, cotton clothing.
- Keep fingernails trimmed short.
- There are rare reports of NSAIDs potentially worsening skin infections in chickenpox, so ibuprofen should be used with caution. In practice, it would be unusual for a child to need ibuprofen if receiving regular paracetamol; pain or pyrexia necessitating its use in addition to paracetamol should prompt consideration of serious bacterial superinfection.
- There is no evidence to support the use of acyclovir in young, immunocompetent children with self-limiting, uncomplicated chickenpox; it does not decrease the incidence of complications.
What to do if you suspect bacterial superinfection
- Otherwise well children with evidence of few, small areas of bacterial superinfection can be managed in the community with oral antibiotics and safety-netting advice.
- Children with evidence of collection, extensive areas of bacterial superinfection, who are unwell, or have other features consistent with possible serious bacterial superinfection, need urgent referral to secondary care.
- In secondary care, unwell children with evidence of shock / sepsis need urgent resuscitation and intravenous antibiotic administration; if possible this should include clindamycin, due to its vital role in inhibiting toxin production by GAS.
- Invasive GAS infection has high mortality, and if suspected there should be a low threshold to involve senior staff, regional PICU services, and in the case of necrotising fasciitis, surgical teams (for early debridement); early use of inotropes and IVIG may also be required.
Bibliography
Chickenpox NICE Clinical Knowledge Summary (which I found to be the best resource by far): http://cks.nice.org.uk/chickenpox
Cohen J, Breuer J. Chickenpox treatment. Systematic review 912. BMJ Clinical Evidence.
Papadopoulos, AJ. Chickenpox. emedicineWebMD. www.emedicine.com
References
Re: “the increased incidence of group A streptococcal (GAS) colonisation in children (around 10% are asymptomatic carriers in the throat or on skin)”
Shaikh N, Leonard E, Martin JM. Prevalence of streptococcal pharyngitis and streptococcal carriage in children: a meta-analysis. Pediatrics. 2010 Sep;126(3):e557-64
Re. “Around a third of children admitted to hospital with chickenpox have secondary skin infection”:
Bovill B, Bannister B. Review of 26 years/ hospital admission for chickenpox in North London. Journal of Infection. 1998;36(suppl1);17-23.
Re: “necrotising fasciitis and toxic shock syndrome (TSS); both are associated with high mortality and morbidity in children.” AND “IVIG may also be required.”
Chuang YY, Huang YC, Lin TY. Toxic shock syndrome in children: epidemiology, pathogenesis, and management. Paediatr Drugs. 2005;7(1):11-25.
Re. “There is evidence that sedating antihistamines offer some benefit”
Tebruegge M, Kuruvilla M, Margarson I. Does the use of calamine or antihistamine provide symptomatic relief from pruritus in children with varicella zoster infection? Archives of Disease in Childhood. 2006:91(12);1035-1036.
Re: (continued from above) “chlorphenamine is licensed for this use.”
BNFC, available at: https://www.medicinescomplete.com/mc/bnfc/current/PHP1934-chlorphenamine-maleate.htm?q=chlorphenamine&t=search&ss=text&tot=40&p=1#_hit
Re: “if possible this should include clindamycin, due to its vital role in inhibiting toxin production by GAS.” (as well as having it drilled in to us by the microbiologists at St Thomas’):
http://emedicine.medscape.com/article/228936-medication#2
September 2014 newsletter published
Warts this month, steroids in Bell’s palsy, a recap of the year for the new trainees and some more edicts from NICE on what not to do. A couple of links to good CPD opportunities too. Do leave comments below.
July 2014 published
Last bit of headaches this month with guidance on management of various primary headaches, including medication overuse headache. Also more on domperidone, psoriasis, respiratory and heart rates to worry about and a link to a new colic summary I’ve put under the Primary Care Guidelines tab. Do leave comments below.
Kawasaki Disease
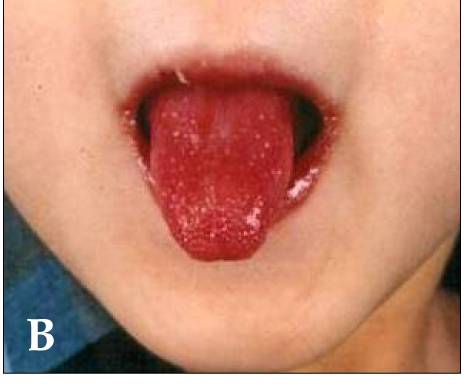
Dr Yasmeen Moin is one of our senior registrars, currently nursing a broken leg and making good use of her time writing accessible articles for Paediatric Pearls! This month she has summarised all the salient points about Kawasaki Disease which is not as rare as people think. Her article is below, under the characteristic “strawberry tongue”.
Kawasaki disease (KD) is an acute febrile childhood vasculitis affecting medium sized arteries, particularly the coronary arteries.
It most commonly affects children aged between 6 months and 4 years, however it can occur in children up to the age of 16.
Diagnosis is based on persistent fever, of 5 days or more, plus 4 of the following:
1) Conjunctivitis – bilateral, bulbar, non suppurative
2) Lymphadenopathy – cervical >1.5 cm
3) Rash – widespread, polymorphous, NOT vesicular
4) Lips and oral mucosa – red cracked lips, “strawberry” tongue, erythematous oral cavity
5) Changes of extremities – erythema, oedema of palms and soles initially, then peeling of skin at a later stage
NB:
Fever is often >39°, remittent and unresponsive to antibiotics and antipyretics.
Incomplete KD can occur where not all diagnostic criteria are met. It is more common in children less than a year old. Think KD when prolonged unexplained fever even if less than four diagnostic criteria.
Children with KD are often extremely irritable. Think KD if fever, irritable and skin manifestations.
KD is often accompanied by concurrent infections which may be misleading.
Why is it important to diagnose?
KD is the commonest cause of acquired cardiac disease in the UK and USA with 25% of untreated cases of KD developing cardiac complications. Timely treatment reduces coronary artery damage by up to 75%. Children less than 1 year of age with incomplete KD have a higher risk of developing cardiac sequelae.
I’ve not seen one before, how common is it?
KD is relatively common with an annual incidence in the UK and United States of approximately 9-12 per 100 000 children under 5 years (compared to an age- matched incidence of meningococcal disease of approximately 1 per 100 000).
What do I need to do?
Children with suspected KD should be referred to the Paediatric team urgently, as early treatment significantly reduces the risk of long term cardiac artery damage.
If there is a high index of suspicion, referral should be made before 5 days of fever.
Diagnosis is clinical; however there are characteristic laboratory findings:
Elevated WBCs, mainly neutrophils
Markedly elevated ESR and CRP
Hypoalbuminaemia
Normocytic, normochromic anaemia
Mildly elevated LFTs, mainly ALT
Normal platelet count that increases markedly in week two of illness
How is it treated?
Treatment involves admission to a paediatric ward and administration of IV immunoglobulin (IVIG). This causes rapid defervescence and clinical improvement in 80% of cases. High dose aspirin is also commenced (dosing regimen will vary according to local policy). A second dose of IVIG may be required if there is no response to the initial dose. Anti-viral IgG in IVIG may interfere with the efficacy of live vaccines.
An ECHO, looking in particular for coronary artery aneurysms, is usually performed during the initial admission and then at 6 weeks (or sooner, again depending on local policy).
Once the fever has resolved, aspirin is continued at a low dose and in those children with a normal ECHO at 6 weeks, it is discontinued.
What follow up should I expect?
Long term, often lifelong, paediatric cardiology follow up is required. Repeat ECHOs are carried out regularly (as per local policy). Lifelong aspirin and anticoagulant therapy may be required if aneurysms persist, if they are >8mm and if stenoses are identified. Further investigations, such as coronary angiography, may need to be carried out. The long term effects of KD on adult coronary disease are unclear but the family should be given advice on minimising atheroma risk factors. Early monitoring of blood pressure and lipids should be considered.
Parents should be reassured that KD is not contagious and that most children make a full recovery without any long term sequelae.
Useful links
http://www.patient.co.uk/health/kawasaki-disease
http://www.racgp.org.au/afp/2013/july/kawasaki-disease/
References
Kawasaki disease. The importance of prompt recognition and early referral Volume 42, No.7, July 2013 Pages 473-476
Surveillance of Complete Kawasaki Disease in the UK and Ireland, RCPCH
Whipps Cross Paediatric Unit Guidelines
http://circ.ahajournals.org/content/110/17/2747.full.pdf+html provides a full text 26 page in-depth discussion on everything to do with Kawasaki Disease. Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease. A Statement for Health Professionals From the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Jane W. Newburger, MD, MPH;Masato Takahashi, MD et al. Circulation. 2004; 110: 2747-2771
August 2013 PDF published
Thermal injuries from a safeguarding point of view this month, updated fever guidelines, quarantine periods for infectious diseases, house dust mite allergy and facial injuries this month as the last in the minor injuries series. Do leave comments below.
BTS 2011 guideline on community acquired pneumonia in children
In October 2011 the British Thoracic Society updated its guidelines on community acquired pneumonia in children. Dr Michael Eyres looked at it in more detail for Paediatric Pearls. He was also part of our local audit team contributing to the national audit. The results showed that we, despite insisting on as few investigations as possible, are still doing too many chest x-rays, blood cultures and CRP measurements. Think – will it change management?
Here are the basics:
When to consider pneumonia
Persistent fever > 38.5°C + chest recessions + tachypnoea
Investigations
• CXR should not be considered routine and is not required in children who do not need admission.
• Acute phase reactants including CRP are not useful in distinguishing viral from bacterial infection and should not
be tested routinely. Blood cultures also do not need to be routinely taken.
• Daily U&Es are required in children receiving IV fluids.
Severity assessment
• Children with oxygen saturations <92% need hospital referral.
• Auscultation findings of absent breath sounds with dullness to percussion need hospital referral.
• Children should be reassessed if symptoms persist.
General management
• Give parents information on managing fever, preventing dehydration and identifying deterioration.
• Children with oxygen saturations <92% need oxygen.
• NG tubes should be avoided in severe respiratory compromise and in infants.
• Chest physio is not beneficial and should not be performed in pneumonia.
Antibiotics
• All children with a clear clinical diagnosis of pneumonia should receive antibiotics as bacterial and viral
infections cannot be reliably distinguished. However most children younger than 2 years presenting with mild symptoms of respiratory distress (this would
include the bronchiolitics) do not usually require antibiotics.
• Amoxicillin is the oral first-line for all children as it is effective, well tolerated and cheap.
• Macrolides if no response to first-line / suspected mycoplasma or chlamydia / very severe disease.
• Augmentin if pneumonia associated with influenza.
• Oral agents are effective even in severe pneumonia; IV is needed only if unable to tolerate oral or there are
signs of septicaemia, empyema or abscess.
Follow-up
• Children with severe pneumonia or complications should be followed up after discharge until they have recovered completely and
CXR is near normal. Follow-up CXR is not otherwise required, but may be considered in round pneumonia, collapse or if symptoms persist.
January 2012 PDF ready
Do you know your valgus from your varus? Or your myclonic epilepsy from your sleep myoclonus? A link this month to new asthma patient information leaflets and some reminders of NICE’s “Do not do recommendations” in feverish children. Also the BSACI egg allergy guideline. Do leave comments on any of these topics below.
Antipyretics – single or dual therapy?
Managing Fever in Children with thanks to Dr Ranjev Kainth
Fever, both in primary and secondary care is a frequent presentation. Often, it is a sign of an illness and in the first instance, it is important to establish the most likely underlying causative factor. Once this has been determined, focus often turns to the management of the fever. Two recent articles in Archives highlight the varying practice amongst clinicians both in primary and secondary care.
In accordance with NICE guidelines1, the authors2-3 suggest anti-pyretics should not be used for the sole purpose of controlling fever. Agents such as paracetamol and ibuprofen are often administered to promote comfort in the child when there is fever. In such situations, children may be prescribed single or dual therapy.
In a systematic review, E.Purssell3 examines the evidence for combined anti-pyretic therapy with either paracetamol or ibuprofen alone. He concluded that ‘only marginal benefit was shown for the combined treatment compared with each drug individually which, taken alongside the risk of overdose and further increasing the fear of fever, suggests there is little to recommend this practice’.
With the real risk of parents being unable to accurately measure medication4, it is important clear guidance is given on when and what type of drug therapy is appropriate in clinical situations.
References:
- NICE Guideline: Feverish Illness in Children: Quick reference guideline http://guidance.nice.org.uk/CG47/QuickRefGuide/pdf/English
- McLyntyre, J. Management of fever in Children. Arch Dis Child Dec 2011 V 96;12 P.1173
- Purssell, E. Systematic review of studies comparing combined treatment with paracetamol and ibuprofen, with either drug alone. Arch Dis Child Dec 2011 V 96;12 P.1175
- Beckett, V.L. et al. Accurately administering oral medication to children isn’t child’s play. Arch Dis Child 2011;96:A7 doi:10.1136/adc.2011.212563.14