Scabies this month with a beautiful picture of plantar lesions in a child. Updated NICE head injuries, antipyretics (or not) for febrile convulsions, child trafficking and the last in the sleep series. Do leave comments below.
Category Archives: For General Practitioners
Dermatology for the New Year!
Eczema this month, a reminder of treatment of infections and links to some useful audit tools from NICE. Next month, scabies. Another excellent website on food and nutrition in toddlers with a bit on do’s and don’ts of faddy eating and a paper on whether treating ADHD reduces crime. Do leave comments.
November/December 2013
Seasonal treats this month in the form of bronchiolitis treatments and the use of antipyretics in febrile convulsions. Perennial subjects include obesity, BCG lymphadenitis and a concise reminder of the management of UTI in children.
Obesity – assessment in secondary care and associated dysmorphisms
Article by Dr Hajera Sheikh, paediatric registrar
Assessment in Secondary Care
History:
• Lifestyle Assessment
• Menstrual History
• Obstructive Sleep Apnoea: Snoring, difficulty breathing during sleep, morning headaches or fatigue
• Symptoms of co-morbidity including psychological
• Drug use (particularly glucocorticoids and atypical antipsychotics)
• Family history, particularly diabetes <40 yrs, early heart disease <60 yrs
Examination:
• Height, weight, BMI
• Obesity pattern: generalised, central (greater risk of adverse cardiovascular outcomes), buffalo hump and neck (may be suggestive of Cushing syndrome)
• Blood pressure
• Pubertal assessment
• Acanthosis nigricans (indicative of insulin resistance, first seen round neck and axillae)
• Signs of endocrinopathy
• Dysmorphisms: (Look out for early onset obesity, learning difficulties, deafness, epilepsy, retinitis, dysmorphic features, hypogonadism)
Investigations (directed)
• Urinalysis
• Thyroid function
• Fasting lipids (total and HDL cholesterol), triglycerides
• Liver function, including ALT
• Fasting glucose and insulin not usually done first line
Refer to Paediatric Obesity/Endocrinology or other specialist service if further investigation is required
Aetiology
• Genetic studies
• Thyroid studies: T3, thyroid antibodies, calcium, phosphate
• Cushing syndrome investigations
For co-morbidities
• Oral glucose test
• PCOS studies (LH, FSH, adrenal androgens, Sex Hormone Binding Globulin, prolactin, pelvic ultrasound)
• Sleep Study
Dysmorphic and monogenic syndromes associated with obesity:
Main clinical obesity associated syndromes:
• Chromosomal
Prader-Willi syndrome
Trisomy 21
• Autosomal dominant
Biemond syndrome (some cases)
• Autosomal recessive
Aistrom syndrome
Bardet-Biedl syndrome
Biemond Syndrome(some cases)
Carpenter syndrome
Cohen syndrome
• X-linked inheritance
Borjeson-Forssman-Lehmann syndrome
• Single gene lesions affecting leptin metaboilsm
Congenital leptin deficiency
Leptin receptor mutation
Prohormone convertase 1 mutation
Melanocortin 4 mutation
Clinical features suggesting obesity may be secondary to another condition or syndrome
• Severe unremitting obesity
• Disorders of the eyes
Colobomata
Retinal problems, especially retinitis pigmentosa
Narrow palpebral fissures
Abnormally positioned palpebral fissures
Severe squint (eg Prader-Willi)
• Skeletal abnormalities
Polydactyly
Syndactyly
Kyphoscoliosis
• Sensorineural deafness (eg Alstrom syndrome: sensorineural deafness, diabetes mellitus, retinal dystrophy, obesity)
• Microcephaly and/or abnormally shaped skull
• Mental retardation
• Hypotonia
• Hypogonadism
Crptorchidism
Micropenis
Delayed puberty
• Renal abnormalities
• Cardiac abnormalities
BCG lymphadenitis
BCG Lymphadenitis with thanks to Dr Mujahid Hassan
Lymphadenitis is the most common complication of BCG vaccination, and is of two types – suppurative and non-suppurative.
Normal course post-vaccination:
Intradermal injection -> local multiplication of vaccine -> transport to lymphatics via lymph glands -> haematogenous dissemination of BCG.
No clear definition of ‘BCG lymphadenitis,’ proposed definition is when it becomes palpable or concerning for parents.
Can appear as early as two weeks after vaccination, most within 6 months and almost all cases will be within 24 months.
Normally ipsilateral with one or two palpable lymph nodes, but can involve multiple nodes. Normally axillary but can be with cervical/supraclavicular.
Diagnosis:
- Isolated lymph node enlargement
- BCG vaccination to ipsilateral side
- Absence of tenderness or heat to lump
- Absence of fever
Non-suppurative will resolve within a few weeks – this is a normal reaction and most of these are sub-clinical so go unnoticed.
Suppurative involves an enlarging lymph node with fluctuant appearances, oedema and erythema. Happens in ’30-80%’ of cases of lymphadenitis.
Treatment of suppurative lymphadenitis:
Antibiotics: Previously erythromycin/rifampicin/isoniazid have been used but their clinical role is of dubious significance, so are not used routinely.
Reassurance and followup are what is needed.
Fine Needle Aspiration: Suppurative lymphadenitis can result in spontaneous perforation and sinus formation, which can result in several unpleasant months of dressing and wound care. FNA is thus recommended to prevent this and reduce time for healing.
Surgical excision: Risks of general anaesthesia – other than in extreme cases of failed FNA/multiloculated lymph nodes – far outweigh the potential benefits.

Non-suppurative
 Suppurative
Suppurative

Management pathway and images courtesy of:
WM Chan, YW Kwan, CW Leung. Management of Bacillus Calmette-Guérin Lymphadenitis, Hong Kong Journal of Paediatrics (New Series). Vol 16. No. 2, 2011, available via http://www.hkjpaed.org/details.asp?id=782&show=1234
References:
J Goraya and V Virdi, Bacille Calmette-Guérin lymphadenitis, Postgrad Med J. 2002 June; 78(920): 327–329,
available via http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1742390/pdf/v078p00327.pdf
October 2013 newsletter
Lots of writing on this month’s PDF digest, much of it thanks to our registrars. Rotavirus oral vaccination, wheezing in the under 2s, bradycardia, conduct disorder, Kawasaki disease and force feeding. Do leave comments below.
Kawasaki Disease
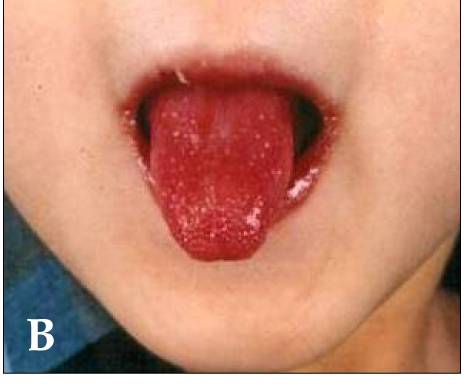
Dr Yasmeen Moin is one of our senior registrars, currently nursing a broken leg and making good use of her time writing accessible articles for Paediatric Pearls! This month she has summarised all the salient points about Kawasaki Disease which is not as rare as people think. Her article is below, under the characteristic “strawberry tongue”.
Kawasaki disease (KD) is an acute febrile childhood vasculitis affecting medium sized arteries, particularly the coronary arteries.
It most commonly affects children aged between 6 months and 4 years, however it can occur in children up to the age of 16.
Diagnosis is based on persistent fever, of 5 days or more, plus 4 of the following:
1) Conjunctivitis – bilateral, bulbar, non suppurative
2) Lymphadenopathy – cervical >1.5 cm
3) Rash – widespread, polymorphous, NOT vesicular
4) Lips and oral mucosa – red cracked lips, “strawberry” tongue, erythematous oral cavity
5) Changes of extremities – erythema, oedema of palms and soles initially, then peeling of skin at a later stage
NB:
Fever is often >39°, remittent and unresponsive to antibiotics and antipyretics.
Incomplete KD can occur where not all diagnostic criteria are met. It is more common in children less than a year old. Think KD when prolonged unexplained fever even if less than four diagnostic criteria.
Children with KD are often extremely irritable. Think KD if fever, irritable and skin manifestations.
KD is often accompanied by concurrent infections which may be misleading.
Why is it important to diagnose?
KD is the commonest cause of acquired cardiac disease in the UK and USA with 25% of untreated cases of KD developing cardiac complications. Timely treatment reduces coronary artery damage by up to 75%. Children less than 1 year of age with incomplete KD have a higher risk of developing cardiac sequelae.
I’ve not seen one before, how common is it?
KD is relatively common with an annual incidence in the UK and United States of approximately 9-12 per 100 000 children under 5 years (compared to an age- matched incidence of meningococcal disease of approximately 1 per 100 000).
What do I need to do?
Children with suspected KD should be referred to the Paediatric team urgently, as early treatment significantly reduces the risk of long term cardiac artery damage.
If there is a high index of suspicion, referral should be made before 5 days of fever.
Diagnosis is clinical; however there are characteristic laboratory findings:
Elevated WBCs, mainly neutrophils
Markedly elevated ESR and CRP
Hypoalbuminaemia
Normocytic, normochromic anaemia
Mildly elevated LFTs, mainly ALT
Normal platelet count that increases markedly in week two of illness
How is it treated?
Treatment involves admission to a paediatric ward and administration of IV immunoglobulin (IVIG). This causes rapid defervescence and clinical improvement in 80% of cases. High dose aspirin is also commenced (dosing regimen will vary according to local policy). A second dose of IVIG may be required if there is no response to the initial dose. Anti-viral IgG in IVIG may interfere with the efficacy of live vaccines.
An ECHO, looking in particular for coronary artery aneurysms, is usually performed during the initial admission and then at 6 weeks (or sooner, again depending on local policy).
Once the fever has resolved, aspirin is continued at a low dose and in those children with a normal ECHO at 6 weeks, it is discontinued.
What follow up should I expect?
Long term, often lifelong, paediatric cardiology follow up is required. Repeat ECHOs are carried out regularly (as per local policy). Lifelong aspirin and anticoagulant therapy may be required if aneurysms persist, if they are >8mm and if stenoses are identified. Further investigations, such as coronary angiography, may need to be carried out. The long term effects of KD on adult coronary disease are unclear but the family should be given advice on minimising atheroma risk factors. Early monitoring of blood pressure and lipids should be considered.
Parents should be reassured that KD is not contagious and that most children make a full recovery without any long term sequelae.
Useful links
http://www.patient.co.uk/health/kawasaki-disease
http://www.racgp.org.au/afp/2013/july/kawasaki-disease/
References
Kawasaki disease. The importance of prompt recognition and early referral Volume 42, No.7, July 2013 Pages 473-476
Surveillance of Complete Kawasaki Disease in the UK and Ireland, RCPCH
Whipps Cross Paediatric Unit Guidelines
http://circ.ahajournals.org/content/110/17/2747.full.pdf+html provides a full text 26 page in-depth discussion on everything to do with Kawasaki Disease. Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease. A Statement for Health Professionals From the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Jane W. Newburger, MD, MPH;Masato Takahashi, MD et al. Circulation. 2004; 110: 2747-2771
September 2013 round-up
The newsletter this month is mainly a round-up of past posts which have been quite useful for ED doctors and GPs. It’s quite hard finding your way around Paediatric Pearls when you first start using it so I hope the articles linked to from this month’s newsletter start you off and give you a flavour of the sort of thing you can find on this website. Thanks to Dr Tom Waterfield who was once a paediatric trainee with us at Whipps and who has now taken over the “From the literature” slot to keep us all up to date with recent relevant publications.
PEWS is not a national score but the idea is worth thinking about nationally. We use it to try to identify the children who are at most risk of becoming more unwell so that measures can be put in place to reverse this trajectory. Remember though, a low PEWS does not necessarily mean the child is safe either. Children need frequent observations when they are in an acute area and staffing levels need to be appropriate to support this.
Do leave any comments on this month’s newsletter below.
August 2013 PDF published
Thermal injuries from a safeguarding point of view this month, updated fever guidelines, quarantine periods for infectious diseases, house dust mite allergy and facial injuries this month as the last in the minor injuries series. Do leave comments below.
July 2013 PDF
Neglect and emotional abuse is the safeguarding topic this month. ED advice on the management of minor head injuries, a report from BPSU in hypocalcaemic fits secondary to vitamin D deficiency, the new UK immunisation poster and a bit on crying babies. Hope you find it all helpful. Comments welcome below