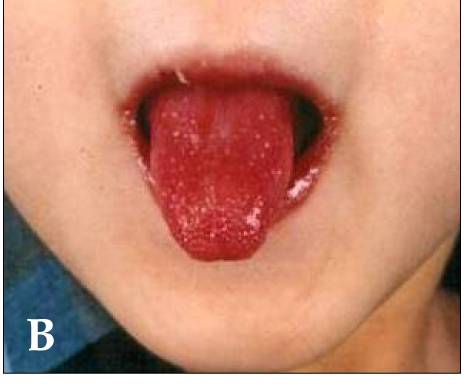
Dr Yasmeen Moin is one of our senior registrars, currently nursing a broken leg and making good use of her time writing accessible articles for Paediatric Pearls! This month she has summarised all the salient points about Kawasaki Disease which is not as rare as people think. Her article is below, under the characteristic “strawberry tongue”.
Kawasaki disease (KD) is an acute febrile childhood vasculitis affecting medium sized arteries, particularly the coronary arteries.
It most commonly affects children aged between 6 months and 4 years, however it can occur in children up to the age of 16.
Diagnosis is based on persistent fever, of 5 days or more, plus 4 of the following:
1) Conjunctivitis – bilateral, bulbar, non suppurative
2) Lymphadenopathy – cervical >1.5 cm
3) Rash – widespread, polymorphous, NOT vesicular
4) Lips and oral mucosa – red cracked lips, “strawberry” tongue, erythematous oral cavity
5) Changes of extremities – erythema, oedema of palms and soles initially, then peeling of skin at a later stage
NB:
Fever is often >39°, remittent and unresponsive to antibiotics and antipyretics.
Incomplete KD can occur where not all diagnostic criteria are met. It is more common in children less than a year old. Think KD when prolonged unexplained fever even if less than four diagnostic criteria.
Children with KD are often extremely irritable. Think KD if fever, irritable and skin manifestations.
KD is often accompanied by concurrent infections which may be misleading.
Why is it important to diagnose?
KD is the commonest cause of acquired cardiac disease in the UK and USA with 25% of untreated cases of KD developing cardiac complications. Timely treatment reduces coronary artery damage by up to 75%. Children less than 1 year of age with incomplete KD have a higher risk of developing cardiac sequelae.
I’ve not seen one before, how common is it?
KD is relatively common with an annual incidence in the UK and United States of approximately 9-12 per 100 000 children under 5 years (compared to an age- matched incidence of meningococcal disease of approximately 1 per 100 000).
What do I need to do?
Children with suspected KD should be referred to the Paediatric team urgently, as early treatment significantly reduces the risk of long term cardiac artery damage.
If there is a high index of suspicion, referral should be made before 5 days of fever.
Diagnosis is clinical; however there are characteristic laboratory findings:
Elevated WBCs, mainly neutrophils
Markedly elevated ESR and CRP
Hypoalbuminaemia
Normocytic, normochromic anaemia
Mildly elevated LFTs, mainly ALT
Normal platelet count that increases markedly in week two of illness
How is it treated?
Treatment involves admission to a paediatric ward and administration of IV immunoglobulin (IVIG). This causes rapid defervescence and clinical improvement in 80% of cases. High dose aspirin is also commenced (dosing regimen will vary according to local policy). A second dose of IVIG may be required if there is no response to the initial dose. Anti-viral IgG in IVIG may interfere with the efficacy of live vaccines.
An ECHO, looking in particular for coronary artery aneurysms, is usually performed during the initial admission and then at 6 weeks (or sooner, again depending on local policy).
Once the fever has resolved, aspirin is continued at a low dose and in those children with a normal ECHO at 6 weeks, it is discontinued.
What follow up should I expect?
Long term, often lifelong, paediatric cardiology follow up is required. Repeat ECHOs are carried out regularly (as per local policy). Lifelong aspirin and anticoagulant therapy may be required if aneurysms persist, if they are >8mm and if stenoses are identified. Further investigations, such as coronary angiography, may need to be carried out. The long term effects of KD on adult coronary disease are unclear but the family should be given advice on minimising atheroma risk factors. Early monitoring of blood pressure and lipids should be considered.
Parents should be reassured that KD is not contagious and that most children make a full recovery without any long term sequelae.
Useful links
http://www.patient.co.uk/health/kawasaki-disease
http://www.racgp.org.au/afp/2013/july/kawasaki-disease/
References
Kawasaki disease. The importance of prompt recognition and early referral Volume 42, No.7, July 2013 Pages 473-476
Surveillance of Complete Kawasaki Disease in the UK and Ireland, RCPCH
Whipps Cross Paediatric Unit Guidelines
http://circ.ahajournals.org/content/110/17/2747.full.pdf+html provides a full text 26 page in-depth discussion on everything to do with Kawasaki Disease. Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease. A Statement for Health Professionals From the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Jane W. Newburger, MD, MPH;Masato Takahashi, MD et al. Circulation. 2004; 110: 2747-2771

 Suppurative
Suppurative